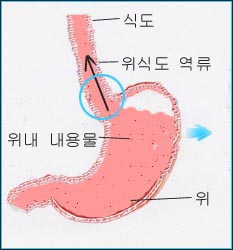
위식도 역류가 있을 때
◯원내에 분문이 있다. 그 분문이 활짝 열려 있다.
출처-소아가정간호백과와 Galaxo Wellcome
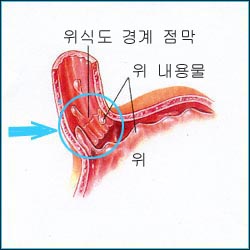
위식도 역류가 거의 없을 때
- 위식도 역류(GER)와 위식도 역류 병(GERD)은 식도 운동성 기능의 부전으로 생기는 것이 보통이다. 모유나 인공영양을 넘길 때 참조.
- 위식도 역류는 영유아들에게 흔히 생기는 생리적 위식도 역류와 병적으로 생기는 병적 위식도 역류 두 종류가 있다.
- 위와 식도 사이에 있는 분문 괄약근이
- 미약하고
- 긴장성이 낮을 때,
- 어떤 이유로 위 내 압이나 복강 내 압이 정상 이상으로 상승될 때,
- 위 내 음식물이나 위액이 비정상적으로 천천히 십이지장 속으로 내려갈 때,
- 그 외 다른 원인으로 분문이 열리고 위 내 내용물이 위 속에서 식도(관) 속으로 역류할 수 있다. 이 경우는 위식도 역류라 하고 그 내용물이 인두강 내, 구강 내로 나올 수 있다. 이 경우를 위식도 역류병이라 한다. 그러나 이 두 경우를 확실히 분간할 수 없는 때도 많다.
- 이런 현상이 경미하고 생리적으로 생기는 경우를 생리적 위식도 역류라 하고 그 정도가 심해 증상이 생기고 합병증이 생기는 경우를 병적 위식도 역류 병 또는 위식도 역류병이라고 한다.
- 위 내용물이 위식도 역류로 분문을 통해서 구강, 인두강까지 올라올 수도 있다. 이런 경우를 기능적 역류(Regurgitation)라고 위 내용물이 분문을 통과해서 식도로만 역류하는 기능적 역류를 잠재성 역류(Occult reflux)라고도 한다.
- 기능적 역류(Regurgitation)는 첫 돌 이전에 아주 흔하다.
- 위식도 역류(GER)는 생후 3~4개월에 40% 정도 생기고 생후 13~14개월에 5% 이하에서 생긴다.
- 생후 3~18세에서 위식도 역류 병(GERD)이 1.8~22% 생긴다고 한다.


위식도 역류
Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
- 생리적 위식도 역류로 신생아들의 85%는 생후 1주까지 먹은 젖이나 인공영양을 가끔 넘길 수 있다.
- 신생아들의 10% 정도가 젖을 넘길 수 있다.
- 아무 치료를 받지 않아도 생후 2세까지 그런 생리적 위 식도 역류의 증상의 60%는 자연히 없어지고 나머지는 4세까지 계속 될 수 있다.
- 경미한 생리적 위식도 역류가 있으면 먹은 젖이나 인공영양을 넘기거나 경미하게 구토할 수 있다.
- 병적 위식도 역류로 인해 위 속에 있는 위 내 내용물이 위 속에서 식도 속으로 역류돼서 여러 가지 증상 징후가 나이에 따라서 다르게 나타날 수 있다.
-
- 신경이 예민하고 음식물 먹기를 싫어하고 재발성 복통, 체중이 증가되지 않고 연하곤란 등이 생길 수 있고 재발성 기능적 역류, 구토, 오목가슴 쓰림 등의 증상 징후가 생길 수 있다.
- 식도염, 기관지 천식, 무호흡증, 서맥(심박이 비정상적으로 서서히 뛰고), 또는 재발성 폐렴이 생길 수 있다.
- 지속성 천식이 있는 비 아토피성 소아들의 3분의 2에서 위식도 역류 병(GERD)이 있고 위식도 역류 병이 잘 치료되어야 천식도 잘 치료된다(출처;Pediatrics News December 2008).
- 구기, 구토, 빈혈, 토혈, 위장출혈, 야간성 기침, 목쉼, 복통, 짜증, 식욕 감퇴, 구취, 고약한 입맛, 입안에서 신 냄새, 사경 등의 증상 징후가 생길 수 있고 드물게는 앞가슴이 뻐근하게 아플 수 있다. 소아 성장 중지증도 생길 수 있다.
- 자다가 깨기도 한다(출처:American Academy of Pediatrics, Guid to Your Child’s Sleeps).
- 등을 활같이 꾸부리고 목을 이상한 위치를 취하기도 하고 사경이 생길 수 있다.
- 병력, 증상 징후, 진찰소견 등을 종합해서 이 병을 진단할 수 있다.
- 필요에 따라, 바륨을 삼키면서 검사하는 위식도 콘트라스트 X-선 사진검사와 상부 위장관과 하부 위장관 콘트라스트 X-선 사진검사, 위식도 섬광조형술 검사, 위식도 초음파검사, 식도 운동성 검사, 식도 내 24시간 산도(pH)검사, 식도위 내시경 검사, 식도 생체조직검사 등으로 진단하기도 한다.
- 전염성 식도염, 호산성 식도염, 영아산통, 심장질환, 만성 중이염, 중추신경 질환, 신진대사 이상, 단백질 알레르기, 신장질환, 사랑 결핍증 등과 감별 진단한다.
- 경미한 위식도 역류는 반 고형 음식물을 적절히 소량 자주 먹고, 먹고 난 후 트림을 잘 시키고 30도 정도 머리와 상체를 하체보다 더 높게 높이고 배를 바닥에 대고 눕혀 치료하기도 한다.
- 다음 히스타민 수용체 길항제(H2RAs/H2 blockers) 중 한가지로 치료하기도 하고
- Cimetidine(Tagamet),
- Zantac (Ranitidine Hcl),
- Pepcid (Famotidine),
- Nizatadine(Axid) 등 히스타민 수용체 길항제(H2RAs/H2 blockers)로 치료하기도 하고,
- 다음 PPIs(Proton pump inhibitors)제 중 한가지로 치료할 수 있다.
- Reglan (Metoclopramide),
- Domperidone (Motilium/Motillium/ Motinorm Costi/Nomit).
- Nexium(Esomeprazole Magnesium), ,
- Prilosec (Omeprazole),
- Lanzoprazole(Prevacid) 등
- 심한 위식도 역류 병은 약 6주간 적극적으로 내과적 치료에 효과가 없으면 외과적 수술 치료도 할 수 있다.
- 지속성 천식이 있는 비 아토피성 소아들의 3분의 2에서 위식도 역류 병(GERD)이 있고 위식도 역류 병을 양성자 펌프 억제제(Proton pump inhibitors)와 위장운동촉진제(Prokineticc agents)로 치료하고 또 필요에 따라 수술로 치료하고 천식 치료약으로 치료 한 결과 지속성 천식이 잘 치료됐다고 한다.
출처 및 참조 문헌
- Pediatrics News. December 2008. P8.
- MD Ney Guide, May 2006
- 그 외 다수
위식도 역류 병의 합병증
- 기관지염,
- 후두염,
- 부비동염,
- 재발성 중이염,
- 치아 미란,
- 미란 식도염
- 식도 협착
- 발레트 식도(Barrett’s esophagus)
- 식도암
- 그 외
|
다음은 “위식도 역류병 백문 백답”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 위식도 역류병 백문 백답
Q. 위식도 역류병과 위식도 역류의 차이점은
A.신생아들이나 영유아들이 모유나 인공영양 또는 음식물을 먹은 후 넘기고 간혹 토하기는 하지만 정상으로 성장 발육하고 기관지 천식 등 합병증이 생기지 않는 생리적 위식도 역류를 그냥 위식도 역류(GER) 또는 생리적 위식도 역류라고 한다.
그러나 영양실조, 호흡기 이상과 호흡기 이상으로 생기는 증상 징후, 식도염, 성장 발육 이상 등의 합병증을 동반하는 위식도 역류를 위식도 역류병(GERD)이라 한다. 이런 위식도 역류병은 병적이다.
Q. 위식도 역류는 얼마나 흔한가?
A.생후 2개월 된 영아들의 50%는 위식도 역류로 적어도 하루 두 번 모유나 인공영양을 넘기고 생후 7개월 된 영아들의 15%는 위식도 역류로 모유나 인공영양을 넘기고 생후 15개월 된 유아들의 1%는 위식도 역류로 먹은 음식물을 넘긴다.
Q. 위식도 역류는 어떻게 생기나
A. 식도의 맨 아래 부분이 위로 연결 되는 부위를 유문이라고 한다. 만삭 신생아들이든 미숙 신생아들이든 식도 하부에 있는 유문의 괄약근이 모유나 인공영양을 먹은 후 정상적으로 긴장되어 유문이 닫혀 위 내 내용물이 식도 속으로 역류되지 않는 것이 보통이다.
그러나 때로는 분문의 괄약근이 잠시 동안 이완될 수 있다. 이때는 위내 내용물이 식도 속으로 역류될 수 있다.
영유아의 등을 바닥에 대고 눕히거나 6개월 이전 신생아나 영아를 아기의 의자에 앉힐 때 위 내 내용물이 식도 하부 쪽으로 밀려갈 때 식도 하부에 있는 분문의 괄약근의 긴장성이 이완될 수 있고 이럴 때 위식도 역류가 생길 수 있다.
또 복강 내 압이 기침이나 다른 이유로 일시적으로 상승되면 식도 하부의 있는 유문의 괄략근이 제대로 닫히지 않을 때는 식도 하부의 유문 괄략근이 열려 위식도 역류가 생길 수 있다.
Q. 위식도 역류병과 감별 진단해야 할 다른 병은?
A. 신진대사 이상으로 생기는 병, 음식물 과민증, 선천성 식도위장 폐쇄 등이다.
Q. 위식도 역류병의 주 증상은 무엇인가?
A. 차단성 무호흡증, 과민, 야간성 기침, 천명, 기관지 천식, 재발성 폐렴, 성장지연 등이다
Q. 식도 산성도 측정 검사는 위식도 역류 진단에 상당한 가치가 있는가
A.위식도 역류가 있는 영아들에게서는 별 가치가 없다.
Q.위식도 역류의 일반적인 진행 경과는?
A. 위식도 역류의 증상 징후는 생후 1-4개월에서 가장 심하게 생기고 생후 10개월에서는 55%가 자연적으로 치료되고 생후 18개월에서는 80%가 자연 치료된다.
그 후부터 소아들이나 성인들은 때로는 그 현상이 생겼다가 없어지고 또 생겼다 또 없어질 수 있다.
Q. 위식도 역류의 가장 흔한 증상 징후는?
A. 먹은 모유나 음식물을 먹은 후에 넘기는 증상이다.
분수같이 힘세게 구토할 때는 위식도 폐쇄, 소장 폐쇄나 우유 단백 알레르기 등을 의심해야 한다.
Q. 위식도 역류로 식도염이 생길 수 있나?
A. 위식도 역류로 식도염이 생길 수 있고 그로 인해 영유아가 울고 짜증내고 과민해질 수 있다.
Q.위식도 역류로 상기도에 어떤 증상징후가 생길 수 있나?
A. 영유아의 인두나 후두 등이 막혀 차단성 무호흡증이 생길 수 있고 천명 또는 협착음이 생길 수 있다. 영아기 이후 아이들에게는 위식도 역류로 목이 쉬고 경련성 크루프의 증상이 생길 수도 있다.
Q. 위식도 역류로 인해서 하기도에 어떤 증상징후가 생길 수 있다?
A. 위식도 역류로 인해서 기관지 천식 발작이 유발될 수 있다.
위식도 역류가 있는 아이들의 50%에 천식이 생길 수 있다.
특히 위식도 역류병으로 밤에 기침을 하면서 천식이 생길 수 있다.
Q. 위식도 역류로 인해서 신경 증상도 생길 수 있다?
A. 위식도 역류로 인해서 발작성 사경과 강직성 후궁반장을 동반하는 신경 증상이 생길 수도 있다. 이런 병을 샌디퍼(Sandifer) 증후군이라고 한다.
Q. 위식도 역류병와 음식물 알레르기와는 어떤 관계가 있는가?
A. 위식도 역류병을 가진 아이들 중 위식도 역류병의 증상징후와 음식물 단백질 알레르기의 증상 징후가 같이 생길 수도 있다.
Q. 장기간 위식도 역류병으로 인한 합병증?
A.위식도 역류병을 가진 아이들의 약 10%는 식도염이 생길 수 있고 식도 협착증, 바레트(Barrett)식도 등이 생길 수 있다.
Q. b영아들이 위식도 역류를 가지고 있지만 잘 크고 아무 증상이 없을 때는 어떻게 치료하나?
A. 반고형 음식물을 더 자주 조금씩 적절히 먹이고 트림을 잘 시키고 시간이 지나면 자연적으로 치료된다.
Q. 증상이 있는 위식도 역류를 가진 영아들은 어떻게 치료하나?
A.반고형 음식물을 좀 더 자주 먹이고 위장운동 촉진(Prokinetics)제로 치료하고 제산제로 치료한다.
Q. 증상이 심한 위식도 역류병은 어떻게 치료하나?
A. 내과적 치료를 적극적으로 해보고 그 치료에 효과 없으면 수술치료를 한다.
Metaclopromide나 Cisapride 등으로 치료하기도 한다.
Q. 증상이 있는 영아들의 위식도 역류는 어떤 약으로 치료하나?
A.단기간 제산제와 Ranitidine 등 약으로 치료한다.
|
다음은 “위식도 역류, 아이 입에 거품이 나옵니다.”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 위식도 역류,아이 입에 거품이 나옵니다.
Q. 40일된 아가입니다.
입가에 침이 자주 보이는거 같은데 자세히 보니 침에 거품이 섞여 있어서 문의 드립니다.
입에 거품이 항상 보글보글 합니다.
자주 모유를 올리는데 올리고 나서 보면 거품이 더 많구요
먹은 후 한참 있다가 올리는 편이라 우유 건더기가 나올때가 많구요
소화 되다가 위 속에서부터 올라오는 거 같아요
올리고 나면 힘들어하구요
A. 로미님
안녕하세요. 좋은 질문을 해주셔서 감사합니다.
자녀의 나이, 성별, 과거 병력, 가족 병력, 진찰소견, 임상검사 등 자세한 정보가 더 많이 있을수록 더 좋은 답변을 드릴 수 있지만 주신 정보를 토대로 답변을 드리겠습니다.
코로 숨 쉬는 대신에 입으로 숨을 쉴 때(구강호흡을 할 때)는 입에서 거품이 더 날 수 있습니다.
어떤 이상이 비강 기도 부분이나 후비공 부위에 있나 알아보십시오.
그리고 위식도 역류로 구토하는지 알아보시고
아직도 문제가 계속 되거나 걱정이 되시면 소아 청소년과에서 진찰 진단을 받으시고 그 문제에 관해 상담하시기 바랍니다.
[부모도 반의사가 되어야 한다– 소아가정간호 백과] 제 3권 신생아, 영유아, 학령기 아이 사춘기 아이 성장발육, 위식도 역류 등을 참조하시기 바랍니다.
질문이 더 있으시면 다시 연락 주시기 바랍니다. 방문해 주셔 감사합니다. 이상원.
Gastroesophageal reflux (GER) and gastroesophageal reflux disease (GERD)
Causes of gastroesophageal reflux and gastroesophageal reflux disease
When gastroesophageal reflux is present
◯There is a chest in the garden. The gate is wide open. Source: Encyclopedia of Pediatric and Family Nursing and Galaxo Wellcome
When gastroesophageal reflux is rare
Gastroesophageal mucosa borderline,
◯There is a heart within the circle. The heart is barely open and the stomach contents are refluxing very little into the esophagus. Source: Encyclopedia of Pediatric and Family Nursing and Galaxo Wellcome
• Gastroesophageal reflux (GER) and gastroesophageal reflux disease (GERD) usually result from impaired esophageal motility. See when passing on breast milk or artificial nutrition.
• There are two types of gastroesophageal reflux: physiological gastroesophageal reflux, which commonly occurs in infants, and pathological gastroesophageal reflux, which occurs pathologically.
• The cardiac sphincter between the stomach and the esophagus
o weak o When tension is low, o When, for any reason, the intragastric pressure or intra-abdominal pressure rises above normal,
o When food or gastric juices in the stomach go down abnormally slowly into the duodenum;
o Other causes may cause the heart to open and the contents of the stomach may reflux from the stomach into the esophagus (tube). In this case, it is called gastroesophageal reflux and its contents can come out into the pharyngeal cavity or into the oral cavity. This case is called gastroesophageal reflux disease. However, there are many times when the two cases cannot be clearly distinguished.
• When this phenomenon is mild and physiological, it is called physiological gastroesophageal reflux disease, and when it is severe and causes symptoms and complications, it is called pathological gastroesophageal reflux disease or gastroesophageal reflux disease.
• Gastroesophageal reflux may cause gastric contents to rise through the heart into the oral cavity and pharyngeal cavity. In this case, functional reflux is called functional reflux, and functional reflux in which gastric contents pass through the heart and only into the esophagus is called occult reflux.
• Functional regurgitation is very common before the first stone.
• Gastroesophageal reflux (GER) occurs in about 40% of children at 3–4 months of age and less than 5% at 13–14 months of age.
• Gastroesophageal reflux disease (GERD) is reported to occur in 1.8 to 22% of children aged 3 to 18 years.
Table. Frequency of gastroesophageal reflux 표. 위식도 역류의 빈도
Source – Mission possible: taking control GERD
Symptoms of gastroesophageal reflux disease
Gastroesophageal reflux Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
• With physiological gastroesophageal reflux, 85% of newborns can occasionally skip milk or artificial nutrition by the first week of life.
• About 10% of newborns can breastfeed.
• Even without treatment, 60% of the symptoms of physiological gastroesophageal reflux spontaneously resolve by the age of 2 years, and the remainder may persist until age 4 years of age.
• Mild physiological gastroesophageal reflux may result in overdose or mild vomiting.
• Due to pathological gastroesophageal reflux, the contents of the stomach in the stomach are refluxed from the stomach into the esophagus, and various symptoms and signs may appear differently depending on the age.
• o Sensitive nerves, aversion to food, recurrent abdominal pain, weight loss, and difficulty swallowing may occur, and symptoms such as recurrent functional reflux, vomiting, and heartburn may occur.
o Esophagitis, bronchial asthma, apnea, bradycardia (an abnormally slow heartbeat), or recurrent pneumonia may occur.
• Two-thirds of non-atopic children with persistent asthma have gastroesophageal reflux disease (GERD), and when gastroesophageal reflux disease is well treated, asthma is also well treated (source; Pediatrics News December 2008).
• Symptoms such as goji, vomiting, anemia, hematemesis, gastrointestinal bleeding, nocturnal cough, hoarseness, abdominal pain, irritability, loss of appetite, bad breath, bad taste, sour smell from the mouth, torticollis may occur, and in rare cases, chest pain. can be sick Stagnation of growth in children may also occur.
• Waking up while sleeping (Source: American Academy of Pediatrics, Guid to Your Child’s Sleeps).
• Arching your back, arching your neck in an odd position, and causing torticollis.
Diagnosis of gastroesophageal reflux and gastroesophageal reflux disease
• This disease can be diagnosed by synthesizing the medical history, symptom signs, and examination findings.
• As needed, gastroesophageal contrast X-ray examination while swallowing barium and upper and lower gastrointestinal contrast X-ray examination, gastroesophageal scintillation examination, gastroesophageal ultrasonography, esophageal motility examination, intraesophageal 24 It is sometimes diagnosed by a time acidity (pH) test, esophageal gastroscopy, and esophageal biopsy.
Differential diagnosis of gastroesophageal reflux disease and gastroesophageal reflux disease
• Differential diagnosis is made for infectious esophagitis, eosinophilic esophagitis, infant colic, heart disease, chronic otitis media, central nervous system disease, metabolic abnormality, protein allergy, kidney disease, and love deficiency syndrome.
Treatment of gastroesophageal reflux and gastroesophageal reflux disease
• Mild gastroesophageal reflux is sometimes treated by eating moderately small amounts of semi-solid food frequently, burping well after eating, raising the head and upper body 30 degrees higher than the lower body, and laying the stomach on the floor.
• Sometimes treated with one of the following histamine receptor antagonists (H2RAs/H2 blockers);
o Cimetidine (Tagamet), o Zantac (Ranitidine Hcl),
o Pepcid (Famotidine),
o It is sometimes treated with histamine receptor antagonists (H2RAs/H2 blockers) such as Nizatadine (Axid),
• It can be treated with one of the following PPIs (Proton pump inhibitors).
o Reglan (Metoclopramide),
o Domperidone (Motilium/Motillium/Motinorm Costi/Nomit). o Nexium (Esomeprazole Magnesium),
o Prilosec (Omeprazole),
o Lanzoprazole (Prevacid), etc.
• Severe gastroesophageal reflux disease can be treated surgically if active medical treatment is not effective for about 6 weeks.
• Two-thirds of non-atopic children with persistent asthma have gastroesophageal reflux disease (GERD) and need to treat gastroesophageal reflux disease with proton pump inhibitors and prokinetic agents. As a result of treatment with surgery and asthma medication, persistent asthma was successfully cured. Sources and References
• Pediatrics News. December 2008. P8.
• MD Ney Guide, May 2006
• And many more Complications of gastroesophageal reflux disease
• bronchitis;
• laryngitis;
• Sinusitis;
• recurrent otitis media;
• tooth erosion;
• Erosive esophagitis
• Esophageal stricture
• Barrett’s esophagus
• Esophageal cancer
• etc
The following is an example of Q&A for health counseling for children and adolescents on the Internet regarding “Gastroesophageal Reflux Disease 100 Questions and Answers”.
Q&A. Gastroesophageal reflux disease
Q. What is the difference between gastroesophageal reflux disease and gastroesophageal reflux disease?
A. Physiological gastroesophageal reflux disease (GER) or physiological gastroesophageal reflux disease (GER) or physiological gastroesophageal reflux disease (GERD), which newborns and infants pass after eating breast milk, artificial nutrition, or food, and occasionally vomit, but grows and develops normally and does not cause complications such as bronchial asthma It is said However, gastroesophageal reflux disease (GERD), which accompanies complications such as malnutrition, respiratory abnormalities and symptoms of respiratory abnormalities, esophagitis, and growth and developmental abnormalities, is called gastroesophageal reflux disease (GERD).
This gastroesophageal reflux disease is pathological.
Q. How common is gastroesophageal reflux?
A. 50% of 2-month-old infants pass breast milk or artificial nutrition at least twice a day due to gastroesophageal reflux, and 15% of 7-month-old infants pass breast milk or artificial nutrition due to gastroesophageal reflux, and 15-month-old infants 1% pass through their food due to gastroesophageal reflux.
Q. How does gastroesophageal reflux occur?
A. The part where the lower part of the esophagus connects to the stomach is called the pylorus. Whether full-term or premature newborns, it is common for the pyloric sphincter in the lower esophagus to be normally tense after feeding with breast milk or artificial nutrition, so that the pylorus is closed so that gastric contents do not regurgitate into the esophagus. However, sometimes the cardiac sphincter can relax for a while. In this case, gastric contents may reflux into the esophagus. When an infant or toddler is laid on their back on the floor or when a newborn or infant before 6 months of age is placed on a baby’s chair, when the contents of the stomach are pushed into the lower part of the esophagus, the tension of the cardiac sphincter in the lower part of the esophagus may be relaxed. Reflux may occur. Also, when intra-abdominal pressure rises temporarily due to coughing or other reasons, when the pyloric sphincter in the lower esophagus does not close properly, the pyloric sphincter in the lower esophagus opens and gastroesophageal reflux may occur.
Q. What other diseases should be differentiated from gastroesophageal reflux disease? A. Diseases caused by abnormal metabolism, food intolerance, and congenital esophageal and gastrointestinal obstruction.
Q. What are the main symptoms of gastroesophageal reflux disease?
A. Obstructive apnea, hypersensitivity, nocturnal cough, wheezing, bronchial asthma, recurrent pneumonia, growth retardation, etc.
Q. Is esophageal acidity test of significant value in diagnosing gastroesophageal reflux? A. Of little value in infants with gastroesophageal reflux.
Q. What is the general course of gastroesophageal reflux?
A. The symptoms of gastroesophageal reflux are most severe at 1–4 months of age, 55% spontaneously resolve at 10 months of age, and 80% spontaneously resolve at 18 months of age. From then on, children and adults can sometimes come and go, then come and go.
Q. What are the most common symptomatic signs of gastroesophageal reflux?
A. It is a symptom that passes after eating breast milk or food. When vomiting violently like a fountain, gastroesophageal obstruction, small intestine obstruction, or milk protein allergy should be suspected.
Q. Can gastroesophageal reflux cause esophagitis?
A. Gastroesophageal reflux can cause esophagitis, which can make infants cry, become irritable and irritable.
Q. What symptoms can occur in the upper respiratory tract due to gastroesophageal reflux?
A. Blockage of the pharynx or larynx in infants and young children may result in obstructive apnea, and wheezing or stenosis may occur. After infancy, gastroesophageal reflux may cause hoarseness and convulsive croup symptoms in children.
Q. What symptoms may occur in the lower respiratory tract due to gastroesophageal reflux?
A. Gastroesophageal reflux can cause bronchial asthma attacks. Asthma can occur in 50% of children with gastroesophageal reflux. In particular, gastroesophageal reflux disease can cause asthma while coughing at night.
Q. Can gastroesophageal reflux cause neurological symptoms?
A. Gastroesophageal reflux may cause neurological symptoms with paroxysmal torticollis and ankylosing hernias. This condition is called Sandifer syndrome.
Q. What is the relationship between gastroesophageal reflux disease and food allergy? A. Among children with gastroesophageal reflux disease, symptoms of gastroesophageal reflux disease and symptoms of food protein allergy may occur together.
Q. Complications from long-term gastroesophageal reflux disease?
A. About 10% of children with gastroesophageal reflux disease can develop esophagitis, esophageal stenosis, and Barrett’s esophagus.
Q. How do you treat b-infants with gastroesophageal reflux, but they are large and asymptomatic?
A. Eat small amounts of semi-solid foods more often and properly, burp well, and it will heal naturally over time.
Q. How are infants with symptomatic gastroesophageal reflux treated?
A. Feed semi-solid foods more frequently, treat with prokinetics and treat with antacids. Q. How is severe gastroesophageal reflux disease treated?
A. Actively try medical treatment, and if the treatment is not effective, surgical treatment is performed. It can also be treated with metaclopromide or cisapride.
Q. What medications are used to treat gastroesophageal reflux in symptomatic infants? A. Short-term treatment with antacids and Ranitidine.
The following is an example of Internet pediatric health counseling Q&A regarding “Gastroesophageal reflux, bubbles in the mouth of a child.”
Q&A. Gastroesophageal reflux, bubbles in the mouth of the child.
Q. My baby is 40 days old. It seems that saliva is often seen around the mouth, but if you look closely, there is foam mixed in the saliva, so please inquire. Always bubbling with bubbles in your mouth. I often breastfeed, but after uploading, there are more bubbles. I tend to upload it after a while after eating, so there are a lot of times when milk comes out. It seems to come up from the stomach as it digests. It’s hard after uploading.
A. Romi Good morning. Thanks for asking a good question. The more detailed information such as the child’s age, gender, past medical history, family history, examination findings, and clinical examination, the better we can give you an answer, but we will give you an answer based on the information you have given us. When you breathe through your mouth (when you breathe through your mouth) instead of breathing through your nose, your mouth may bubble more. Find out if there are any abnormalities in the nasal airways or posterior nostrils
And find out if you’re vomiting with gastroesophageal reflux If the problem still persists or if you are concerned, please consult a pediatrician and discuss the problem.WWW.DRLEEPEDIATRICS.COM- Please refer to Volume 3 Newborns, Infants, School-age Children, Growth and Development of Adolescents, Gastroesophageal Reflux, etc. If you have any more questions, please feel free to contact us again. Thank you for visiting. Lee Sang-won.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서