설사와 감염병의 일반적 치료, General basic treatments for diarrhea and infections
영유아들, 학령기 아이들이 위장염으로 구토나 설사를 조금 할 때 치료 Treatment for mildly vomiting and/or diarrhea in infants, toddlers, school children
- 영아들, 유아들, 학령기 아이들이 위장염으로 구토나 설사를 조금 할 때 일률적으로 치료할 수 없다.
- 예를 들어 영유아들이나 학령기 아이들에게 생긴 구토 및, 또는 설사의 일반적 치료법을 설명한다. 영유아들이나 학령기 아이들의 위장염으로 생긴 설사 및, 또는 구토를 치료하는 방법은 하나의 식이 의술이고 인술이다.
- 그때그때 구토 및, 또는 설사의 원인, 증상 및 징후, 중증도에 따라 치료 한다.
- 가령, 바이러스 위장염으로 구토나 설사를 경미하게 하고, 전반적으로 건강하면, 첫 2~4시간 동안 어떤 종류의 음식물이든 경구로 일절 먹이지 말고 관찰 치료를 해도 된다. 그러나 모유를 먹는 영아들에게는 모유수유는 계속 할 수 있고 경구용 페디아라이트 등 포도당 전해질 용액은 의시의 지시에 따라 조금씩 먹일 수 있다. ㄱ.
- 구토나 설사를 심하게 하지 않고, 많이 아프지도 않으면, 경구용 포도당 전해질용액 1회분 용량 30~120cc 정도를 매 2~4시간 간격으로 치료를 시작 첫 12~24시간 동안 조심스럽게 먹어 현상유지 수화치료를 계속 할 수 있다. 단, 이런 치료를 시작하기 전에 가능한 한 의사의 지시에서 따라 한다.
- 그 다음, 구토와 설사를 더 이상하지 않고, 많이 아프지 않으면, 유당이 섞이지 않은 인공영양이나 소고기 국물이나 닭고기 국물, 사과즙 등 위장에 자극성이 거의 없는 반 유동 음식물이나 또는 페디아라이트 등 포도당 전해질 수화치료 용액 등 전 유동 음식물 중 한두 가지를 골라 1회분 량 30~90cc 정도를, 매 2~4시간 간격으로 12~24시간 동안 먹여 현상유지 수화치료를 해본다.
- 이런 반 유동 음식물 또는 전 유동 음식물 경구 섭취 치료를 하는 동안 설사나 구토를 덜 하면 매 1회분 량을 섭취할 때마다 유동 음식물 15~30cc 정도를 바로 전 섭취 했던 용량 보다 더 증가시켜 섭취한다.
- 이런 식으로 12~24시간 동안 유동 음식물 섭취로 현상 유지 수화 치료를 계속 한다.
- 이때 구토와 설사를 더 이상 하지 않든지, 전반적으로 구토나 설사의 정도가 덜 하면 전 유동 음식물에서 반 유동 음식물로 점차로 바꾸어 주든지 반 유동 음식물에서 보통 때 먹는 음식물로 점차로 바꿔 조금씩 먹이기 시작한다.
- 계속 점차로 나아가면, 그 다음은, 평소 먹었던 음식물을 한두 끼니 먹여본 후 설사 구토를 더 이상 하지 않으면 그 때부터는 평소에 먹던 음식물로 완전히 바꾸어 먹는다.
- 이런 치료도 어디까지 의사의 지시에 따라 한다.
표 5. 수액 용적 비교표
| 용적 비교표 | |||
| 1 티스푼 | 5cc | – | – |
| 1 테이블 스픈 | 15cc | – | – |
| 4 테이블 스푼 | 1/4컵 | 60cc | – |
| 8 테이블 스푼 | 1/2컵 | 120cc | – |
| 16 테이블 스푼 | 1컵 | 240cc | – |
| 2 컵 | 1파인트 | ||
| 4 컵 | 1쿼터 | 960cc | – |
| 2 쿼터 | 1/2 갤런 | – | – |
| 1 온스 | 30cc | – | – |
| 4 스틱(1파운드) | 2컵 | 1 파인트 | – |
| 1 컵 | 240cc | 1/2파운드 | 8온스 |
| 1 리터 | 1,000cc | – | – |
| 조금씩 먹는다. 또는 많이 먹는다.’ 등 말 대신, 가능하면 몇 CC, 몇 차 수저, 수저 또는 15 CC 등 정확한 용적 단위를 써서 음식물의 양이나 포도당 전해질 용액 또는 약물의 양을 정확 하게 표시한다. |
모유를 먹는 영아들의 경미한 설사의 치료Treatment for mild diarrhea of breastfeeding infant

사진 102. 젖 먹는 아이가 경미하게 설사를 하지만 토하지 않으면 모유수유를 보통 때와 같이 계속 할 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
- 젖을 먹는 영아들이 설사를 경미하게 하지만 대체적으로 건강한 것 같고, 보채지도 않고 열이 나지도 않고 탈수되지 않았으면 모유를 계속 수유해도 된다.
- 수유모는 음료수를 보통 때보다 더 많이 섭취하고 더 많이 휴식을 취하면서 가능한 한 모유를 더 충분히 먹인다.
- 젖 먹는 아기가 구토 및, 또는 설사를 하면서 계속 앓을 때도 물론이고 설사 구토를 더 이상 하지 않는 날부터 적어도 2~3일 동안 유당이 들은 인공영양이나 또는 우유 음식물을 먹여서는 안 된다.(만성 비 특이성 영아설사 참조)
- 구토와 설사를 하면서 계속 앓든지, 심하게 앓는 것 같든지, 열이 나든지, 또는 어떻게 수화 치료를 할지 확실히 모르면 의사의 지시에 따라 입원 치료한다.
- 드물게 수유모가 섭취한 음식물 성분이 모유로 분비될 수 있다. 그 음식물 성분이 들은 어마의 젖을 먹는 영아에게 음식물 알레르기가 유발될 수 있고 그로 인해 젖 먹는 영아가 설사 할 수 있다. 수유모가 그런 알레르기 유발 음식물을 섭취해서는 안 된다. [부모도 반의사가 되어야 한다-소아가정간호 백과]-제 4권 모유, 모유수유, 이유-젖 먹는 아기가 아플 때 참조.
영아들이나 유아들, 학령기 아이들에게 생긴 심한 구토 및, 또는 설사로 인한 탈수 치료 Treatment for dehydration due to vomiting and, or diarrhea of infants, toddlers, and school children
- 영아들이나 유아들, 학령기 아이들이 위장염으로 구토 및, 또는 설사로 심하게 탈수될 때는 병원 입원 치료를 받아야 한다.
- 영아들, 유아들, 학령기 아이들의 심한 구토 설사로 생긴 탈수 치료의 예를 들어 설명한다.
영아들이나 유아들, 학령기 아이들에게 생긴 심한 구토 및, 또는 설사로 생긴 탈수 병원 치료

사진 103. 심한 구토 및, 또는 설사로 탈수가 되고 심하게 앓으면 응급 치료를 받아야 한다. 때로는 구급차로 병원 응급실로 가서 치료 받는다.
Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
- 포도당 전해질 용액 정맥주사로 재수화 치료와 현상유지 수화치료를 우선 적절히 하고 탈수가 더 이상 되지 않게 예방적 탈수 치료를 한다.
- 그와 동시에 구토와 설사도 치료한다.
- 입원 치료를 시작한 후 적어도 첫 12~24시간 동안은 음식물을 경구로 일절 먹이지 말아야 한다.
- 그러나 포도당 전해질 용액 정맥주사 재수화 치료를 하는 동시 경구용 포도당 전해질 용액 재수화 현상유지 치료를 한다.
- 1회 분량 30~90cc을 나이에 따라 중증도에 따라 경구로 먹이는 수화 치료를 동시에 할 수 있다.
- 그 다음은, 포도당 전해질 용액 정맥주사로 재수화 치료와 현상유지 수화치료를 계속하면서 경구용 포도당 전해질 재수화 및 현상유지 치료 용액 1회분 30~90cc를 매 2~4시간 간격으로 치료 시작 12~24시간 동안 더 주어 수화치료를 계속 할 수 있다.
- 정맥 주사용 포도당 전해질 용액 수화 치료와 경구용 포도당 전해질 용액으로 재수화 치료를 시작 후 처음 몇 시간 동안 하는 중 구토 설사를 더 이상 하지 않으면 매번 경구용 재수화와 현상유지 수화치료를 할 때마다 그 경구용 수화와 재수화 치료 용액을 30cc 정도를 바로 전 주었던 용량보다 더 증가시켜 준다.
- 나이에 관계없이 경구용 용액 1회 분량은 120~240cc 이상 넘지 않게 한다.
- 이런 식으로 나이와 증상 징후에 따라 경구용 포도당 전해질 용액을 매 2~4시간 간격으로 12~24시간 동안 경구로 주어 재수화 치료 및 현상유지 수화치료를 한다.
혈 중 나트륨 이온(Na⁺)의 농도에 따라 탈수증을 다음과 같이 분류한다.
|
표 32. 영유아들의 탈수 중증도 평가
| 탈수의 정도 | |||
| 관찰 또는 검진 내용 | 경도 탈수증(5%) | 중등도 탈수증(10%) | 중증 탈수증(15%) |
| 일반적 상태 | 갈증, 불안, 흥분 | 갈증, 불안, 과민 반응 | 위축, 기면, 혼수, 빠르고 깊은 호흡 |
| 맥박 | 정상이고 | 빠르게 | 더 빠르게 |
| 맥박 상태 | 정상이고 | 약하고 | 약하고 촉지하기 어렵고 |
| 대천문을 만져보면 | 정상이고 | 움푹 드러가고 | 상당히 더 움푹 드러가고 |
| 눈 | 정상이고 | 움푹 들어가고 | 더 움푹 들어가고 |
| 울 때 눈물 | 눈물이 나고 | 눈물이 나지 않고 | 눈물이 나지 않고 |
| 점막과 입술 상태 | 약간 마르고 | 마르고 | 더 마르고 |
| 피부 긴장도 | 정상이고 | 감소되고 | 더 감소되거나 텐트된다 |
| 피부를 만지면 | 정상이고 | 건조하고 | 친친한 감이 있다 |
| 소변 | 양이 정상적일 수 있다 | 양이 감소되고 농도가 높다 | 몇 시간동안 소변을 보지 않는다 |
| 모세혈관이 채워지는 시간 | 정상 | 2초 이내 | 3초 이상 걸인다 |
| 체중 감소 | 4~5% | 6~9% | 10% 이상 |
출처: Infectious Diseases In Children P18, Vol 17 #5 May 2004 & CDC
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
표 33. 등장성 탈수증, 저장성 탈수증, 고장성 탈수증의 증상 징후
Symptoms, signs of isotonic dehydration, hypotonic dehydration and hypertonic dehydration
| – | 등장성 탈수증 | 저장성 탈수증 | 고장성 탈수증 |
| 혈청 나트륨(Na+)의 농도(mEq/L) |
혈청 나트륨 이온(Na⁺)의 농도 |
혈청 나트륨 이온(Na⁺)의 농도 |
혈청 나트륨 이온(Na⁺)의 농도 |
| 피부 색 | 회색(gray) | 회색(gray) | 회색(gray) |
| 피부의 온도 | 차다 | 차다 | 차다 |
| 피부의 팽만감 turgor | 비 정상 | 상당히 비정상 | 조금 비정상 |
| 촉감 | 건성 | 촉촉한 감 | 밀가루 반죽을 만지는 것과 같은 촉감 |
| 점막 | 마름 | 마름 | 바싹 마름 |
| 눈이 움푹 꺼진다 | 꺼진다 | 꺼진다 | 꺼진다 |
| 숨구멍을 만질 때 | 움푹 들어가 있다 | 움푹 들어가 있다 | 움푹 들어가 있다 |
| 정신상태 | 나쁘다 | 나쁘다 | 아주 나쁘다 |
| 혈압의 감소 | 다소 감소된다. | 다소 감소된다. | 많이 감소된다. |
경증 탈수의 증상 징후
- 기운이 없고,
- 소변 양이 줄고,
- 소변보는 간격이 보통 때보다 길고,
- 소변보는 횟수도 비정상적으로 줄어들고
- 갈증
표 29 각 증상이나 병에 따른 100칼로리 당 필요한 1일 수분과 Na⁺, K⁺ 전해질 이온의 필요량
Average water and electrolyte requirements per 100 calories per 24 hours
| 병명, 증상, 임상적 상태 | H2O (물) (mL) | Na+ mEq | K+ mEq |
| 평균 장관 외 수액 필요량 | 100-120 | 2-4 | 2-3 |
| 문요증 | 45 | 0 | 0 |
| 급성 중추신경 감염과 염증 | 80-90 | 2-4 | 2-3 |
| 요붕증 | 400까지 | 그때그때에 따라 변함 | 그때그때에 따라 변함 |
| 과도 호흡 | 120-210 | 2-4 | 2-3 |
| 열 스트레스 | 120-240 | 그때그때에 따라 변함 | 그때그때에 따라 변함 |
| 고습 환경 | 80-100 | 2-4 | 2-3 |
- 이렇게 포도당 전해질 용액 정맥주사로 재수화 치료 및 현상유지 수화 치료를 하는 동안, 설사 구토 복통 등의 증상 징후도 없고 중증도가 전반적으로 호전되면 정맥주사 포도당 전해질 용액 재수화 현상유지 치료의 용량을 점점 줄이다가 포도당 전해질 용액 주사를 마지막으로 끊는다.
- 그와 반대로 경구용 포도당 전해질 용액의 현상유지 치료용량은 점차로 더 증가시킨다.
- 그 후 구토 설사를 더 이상하지 않을 때는 주사용 포도당 전해질 용액이나 경구용 포도당 전해질 용액을 더 이상 주지 않는다.
- 이때부터는 모유만 먹이든지, 유당이 들지 않은 인공영양만 먹이든지, 쇠고기 국물, 또는 닭고기 국물 등 반 유동 음식물이나 전 유동 음식물 중 한두 가지를 나이에 따라 선택해서 그 다음 12~24시간 동안 조심스럽게 먹는다.
- 그 다음 구토 설사 복통의 증상 징후가 거의 없든지, 조금 있지만 위장염이 거의 회복되어가는 단계에서 유당이 없는 인공영양이나, 쌀죽 등 반 유동 음식물을 소량 한두 번 정도 주다가 구토, 설사, 탈수 등 위장염의 증상 징후가 완전히 없고 건강할 때 평소 먹었던 보통 음식물을 먹기 시작한다.
- 이런 식으로 치료하기 위해 2~3일 동안 또는 그보다 더 오랫동안 병원에서 입원 치료 받는 것이 보통이다.
- 위장염이 다 나은 후 처음 2~3일 동안, 때로는 1~2주 동안은 우유나 우유가 들은 음식물이나 유당이 들은 음식물을 먹지 않는다.
- 물론 원인도 동시 치료한다.
- 이런 치료는 전문적 구토 설사 탈수 치료에 속하지만 부모가 알아야 한다. 그리고 의사의 지시에 따라 한다.
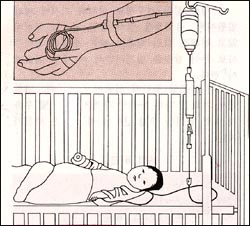
그림 104. 구토 설사 등으로 심히 탈수되면 포도당 전해질 용액주사로 치료한다.
설사와 구토를 치료하는 경구용 전해질 용액의 종류와 성분 Kind and composition of oral electrolytes solutions for treatment of diarrhea and, or vomiting
- 소아청년들 특히 영유아들의 설사, 구토, 탈수, 위장염 등을 치료할 때 이용할 수 있는 경구용 포도당 전해질 용액을 이용할 수 있다.
- 구토, 설사 탈수를 치료할 때 쓸 수 있는 전해질 용액에는 경구용과 혈관용, 드물게는 골수 주사용도 있다.
- 경구용 포도당 전해질 용액은 탈수를 치료할 때 재수화 치료를 하기 위해, 또는 현상유지 수화치료를 하기 위해 사용되는 것이 보통이다.
① 경구용 포도당 전해질 용액으로 구토와 설사 수화 치료 Hydration treatment with oral glucose
electrolytes solution for vomiting and, or diarrhea
- 소아청소년들, 특히 영유아가 경미한 위장염으로 경미하게 구토 및, 또는 설사를 하고 경도로 탈 수될 때 가정에서 부모들이 경구용 포도당 전해질 용액으로 경구 수화치료를 시작할 수 있다.
- 경구용 재수화 치료 또는 현상유지 수화치료 용액을 경구용 포도당 전해질 용액, 이온 액, 또는 이온수라고 한다.
- 용액 대신 포도당 전해질 분말제도 있다.
- 의사의 처방 없이 경구용 포도당 전해질용액을 약국에서 구해 거기에 쓰여 있는 용법에 따라 경미한 설사, 구토, 탈수가 어린 여유아 자녀들에게 생길 때 가정에서 쓸 수 있다.
- 또 가정에서 경구용 설탕 전해질 용액을 의사의 처방에 따라 만들어 위장염으로 생긴 탈수를 치료할 수 있다(표 3 참조).

사진 101. 페디아라이트는 일종의 경구용 포도당 전해질 용액이다.
구토 및, 또는 설사로 생긴 탈수 등의 증상이 있을 때 재수화 치료 또는 현상유지 수화치료를 할 때 쓸 수 있다.
거의 비슷한 경구용 포도당 전해질 용액이 많이 있다. 그리고 의사의 처방이 없이 약국이나 슈퍼마켓에서 사서 쓸 수 있다(표3 참조).
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
표 3. 급성 설사와 탈수의 치료에 쓸 수 있는 경구용 전해질 재수화, 현상유지 수화 용액.
| 경구용 포도당 전해질 용액의 종류 | Na+ in nM/L | K+ in nM/L | Cl– in nM/L | HCO3– mEq/L | 포도당/L(%) | mosM |
| 설사와 탈수를 응급으로 치료할 때 주로 쓰는 경구용 재수화 용액 | ||||||
| WHO에서 권장하는 경구용 재수화 용액(Oral Rehydration Solution) | 90 | 20 | 80 | 30 | 111(2%) | 310 |
| 리하이드라라이트 용액(Rehydralyte solution) | 75 | 20 | 65 | 30 | 139(2.5%) | 305 |
| 탈수가 더 이상 되지 않게 할 때 쓰는 경구용 현상 유지 용액(경구용 포도당 전해질 용액) | ||||||
| 인파라이트 (Infalyte)(Pennwalt 회사) | 50 | 20 | 40 | 30 | 111(2%) | 270 |
| 페디아라이트 용액(Pedialyte)(Ross 회사) | 45 | 20 | 35 | 30 | 139(2.5%) | 250 |
| 라이스라이트 용액(Ricelyte)(Mead Johnson 회사) | 50 | 25 | 45 | – | 3(%) | – |
| 재수화 용액이나 현상유지 용액으로 써서는 안 되는 전 유동식의 종류와 성분 | ||||||
| 가타라데 (Gatarade) | 23 | 3 | 17 | 3 | 255 | 330 |
| 콜라(Cola) | 2 | 0.1 | 2 | 13 | 730 | 750 |
| 쿨에이드(Kool-Aid) | 3 | 0.1 | 0 | 0 | 105 | 465 |
| 사과주스 (apple juice) | 3 | 28 | 30 | 0 | 690 | 725 |
| 하이시(Hi-C) | 2 | 5 | 0 | 0 | 800 | 816 |
| 폽씨클 (popsicle) | 5 | 0.5 | 0 | 0 | 710 | 719 |
| 닭고기 국물 (chicken broth) | 251 | 8 | 250 | 0 | 0 | 501 |
| 맹물 | 0 | 0 | 0 | 0 | 0 | – |
주: 적절한 현상 유지 수화 치료용액은 5-10% Dextrose와 0.2% NaCl + 20 mEq/L KCl 또는 K acetate이다.
참고: 경구용 포도당 전해질 현상유지 용액과 재수화 용액은 비 의료인들이 의사의 처방 없이 약국이나 수퍼마켓트에서 사서 쓸 수 있게 법으로 정하면 좋을 것이라고 생각한다.
표 30. 각종 체액의 전해질 이온 성분, 수소이온 농도(pH)와 삼투압 Electrolytes, pH, Osmolarity of body fluids
| 혈액이나 체액 | Na+ | K+ | Cl– | HCO3– | pH | 삼투압 |
| 위액 | 50 | 10~15 | 150 | 0 | 1 | 300 |
| 췌장액 | 140 | 5 | 50~100 | 100 | 9 | 300 |
| 담즙 | 130 | 5 | 100 | 40 | 8 | 300 |
| 회장루조성 개구 에서 얻은 장액 |
130 | 15~20 | 120 | 25~30 | 8 | 300 |
| 설사변 | 50 | 35 | 40 | 50 | 알카리성 | |
| 땀 | 50 | 5 | 55 | 0 | – | – |
| 혈액 | 140 | 4~5 | 100 | 25 | 7.4 | 285~295 |
| 소변 | 0~100 | 20~100 | 70~200 | 0 | 4.5~8.5 | 50~1400 |
- 표 30에서와 같이 각 계통의 각 기관 속 체액의 전해질의 성분, 이온 농도가 다르다.
- 특히 각 기관의 체액의 전해질 성분 중 K⁺, H⁺, Cl⁻, Na⁺, HCO3⁻등의 성분이 정상적으로 다르다.
- 설사를 할 때, 땀을 많이 흘릴 때, 어떤 전해질이 얼마나 상실되었는지 고려하면서 탈수의 치료에 임하는 것이 보통이다.
- 설사로 탈수 됐을 때 전해질이 거의 들어있지 않는 맹물이나 보리차 물로 설사나 구토로 생긴 탈수를 치료해서는 안 된다.
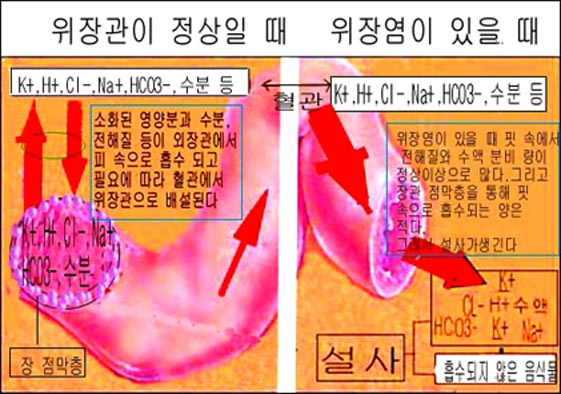
그림 90.장관벽 점막층이 손상되거나 부어서 설사를 할 때
|
◆ 출처 및 참조문헌 참조 ① 급성 탈수증 (Acute dehydration) ② 각 계통의 기관 내 체액의 전해질 성분, pH와 삼투압 (Electrolytes, pH, osmolarity of body fluids) ③ 등장성 탈수 (Isotonic dehydration) ④ 영유아의 탈수의 정도 평가 (Dehydration evaluation in infants and children) ⑤ 등장성 탈수증, 저장성 탈수증, 고장성 탈수증의 증상 징후 ⑥ 설사와 탈수 치료에 쓸 수 있는 급성 탈수증 (Acute dehydration) 경구용 재수화 용액(Oral rehydration solution), 경구용 현상 유지 용액(Oral maintenance solution), 전 유동 음식물(Clear liquid diets) 등의 전해질 농도, 포도당 농도, 삼투압의 비교표 ⑦ 100 칼로리 당 필요한 1일 수분과 전해질의 필요량 (Average water and electrolyte requirements per 100 calories per 24 hours) ⑧ 산성혈증(산혈증) (Acidosis) ⑨ 설사, 구토로 인한 급성 탈수증 (Acute dehydration due to diarrhea, vomiting) ⑩ 설사 및, 또는 구토의 원인과 기전 (Causes and mechanism of diarrhea and/or vomiting) ⑪ 감염병으로 인한 설사와 구토 ⑫ 설사할 때의 음식물 ⑬ 설사 구토와 약물 치료 (Drug treatments for diarrhea and vomiting) ⑭ 경구 수분공급 전해질 용액 (Oral hydration electrolyte solutions) |
General basic treatments for diarrhea and infections
Treatment for mildly vomiting and/or diarrhea in infants, toddlers, school children
• There is no one-size-fits-all treatment for gastroenteritis in infants, toddlers, and school-age children with minor vomiting or diarrhea.
• Describe the general treatment of vomiting and/or diarrhea, for example in infants or school-age children. A method to treat diarrhea and/or vomiting caused by gastroenteritis in infants and young children or school-age children is a dietary medicine and ninjutsu.
• Treat on a case-by-case basis depending on the cause, symptoms and signs and severity of vomiting and/or diarrhea.
• For example, if you have mild vomiting or diarrhea with viral gastroenteritis and are generally healthy, you may be treated by observation without any food of any kind orally for the first 2-4 hours. However, breastfeeding infants can continue breastfeeding, and a glucose electrolyte solution such as oral pedialite can be fed little by little according to the doctor’s instructions. G.
• If vomiting or diarrhea is not severe and is not very painful, take 30~120cc of oral glucose electrolyte per serving every 2~4 hours and carefully eat for the first 12~24 hours to maintain the status quo. can continue However, before starting such treatment, if possible, follow your doctor’s instructions.
• Then, if vomiting and diarrhea are no longer aggravated and painful, lactose-free artificial nutrition, semi-liquid food with little irritation to the stomach, such as beef broth, chicken broth, or apple juice, or glucose electrolyte hydration therapy such as Pedialite Choose one or two of all liquid foods, such as solutions, and feed them at 30~90cc per serving, every 2~4 hours for 12~24 hours, and try the status quo hydration treatment.
• If there is less diarrhea or vomiting during oral intake of such semi-fluid food or full liquid food, take 15-30cc of liquid food at each serving, increasing the amount of liquid food more than the previous intake.
• Continue the status quo hydration treatment with fluid intake in this manner for 12 to 24 hours.
• At this time, if vomiting and diarrhea are no longer present, or if the overall degree of vomiting or diarrhea is less, gradually change from full liquid food to semi-fluid food, or gradually change from semi-fluid food to regular food and start feeding little by little.
• If you keep going gradually, then, after eating one or two meals of your usual food, if you no longer have diarrhea and vomiting, then completely change to your usual food from then on.
• Follow the doctor’s instructions to the extent that such treatment is performed.
Table 5. Fluid volume comparison
표 5. 수액 용적 비교표
| Volume comparison table | |||
| 1 teaspoon | 5cc | – | – |
| 1 tablespoon | 15cc | – | – |
| 4 tablespoon | 1/4 cup | 60cc | – |
| 8 tablespoon | 1/2 cup | 120cc | – |
| 16 tablespoon | 1 cup | 240cc | – |
| 2 cup | 1 pint | ||
| 4 cup | 1 quarter | 960cc | – |
| 2 quarter | 1/2 gallon | – | – |
| 1 oz. | 30cc | – | – |
| 4 sticks (1 pound) | 2 cup | 1 pint | – |
| 1 cup | 240cc | 1/2 pound | 8 oz. |
| 1 liter | 1,000cc | – | – |
Eat little by little Or eat a lot.’ If possible, accurately indicate the amount of food, glucose electrolyte solution, or drug by using precise volumetric units such as several CCs, several spoons, spoons, or 15 CCs.
Treatment for mild diarrhea of breastfeeding infant
Photo 102. As long as the nursing infant has mild diarrhea but does not vomit, breastfeeding can continue as usual. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
• Breastfeeding may continue as long as breastfeeding infants have mild diarrhea but appear generally healthy, do not feel nauseous, do not have a fever, and are not dehydrated.
• Nursing mothers drink more fluids than usual, get more rest, and breastfeed as much as possible.
• Do not feed lactose-containing artificial nutrition or milk foods for at least 2 to 3 days from the day the infant is vomiting and/or continues to suffer from diarrhea, as well as from the day the diarrhea/vomiting ceases. See specific infant diarrhea)
• If you continue to feel sick with vomiting and diarrhea, or if you feel very ill, have a fever, or if you are not sure how to treat hydration, follow your doctor’s instructions to hospitalize.
• Rarely, food components consumed by a nursing mother may be excreted into breast milk. Ingestion of the food ingredients can cause food allergies in infants fed mother’s milk, which in turn can cause diarrhea in the suckling infants. Nursing mothers should not consume such allergens. www.drleepediatrics.com – Volume 4 Breastfeeding, Breastfeeding, Weaning – When a nursing baby is sick.
Treatment for dehydration due to vomiting and, or diarrhea of infants, toddlers, and school children
• Infants, toddlers, and school-age children should be hospitalized if they become severely dehydrated with vomiting and/or diarrhea from gastroenteritis.
• Give examples of treatment of dehydration caused by severe vomiting diarrhea in infants, toddlers, and school-age children. Hospital treatment for dehydration caused by severe vomiting and/or diarrhea in infants, toddlers and school-age children
Photo 103. If you become dehydrated due to severe vomiting and/or diarrhea and become seriously ill, you should seek emergency treatment. Sometimes they go by ambulance to the hospital emergency room for treatment. Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
• Treatment of rehydration and maintenance of the status quo by intravenous injection of glucose electrolyte solution should be performed first and preventive dehydration treatment should be performed to prevent further dehydration.
• Treat vomiting and diarrhea at the same time.
• After initiating inpatient treatment, no food should be given orally for at least the first 12 to 24 hours.
• However, intravenous rehydration therapy with glucose electrolyte solution and oral glucose electrolyte solution rehydration status quo therapy should be administered.
• Hydration treatment can be administered at the same time by oral feeding of 30~90cc per dose depending on age and severity.
• Next, while continuing the rehydration treatment and status quo hydration treatment with intravenous glucose electrolyte solution, 30~90cc of oral glucose electrolyte rehydration and status maintenance treatment solution is administered every 2~4 hours every 2~4 hours 12~ Hydration therapy can be continued by giving an additional 24 hours.
• Vomiting and diarrhea during the first several hours after initiating intravenous glucose electrolyte solution hydration therapy and oral glucose electrolyte solution rehydration therapy with each oral rehydration and status quo hydration therapy. Increase the oral hydration and rehydration treatment solution by 30cc more than the dose given just before.
• Regardless of age, one dose of oral solution should not exceed 120~240cc.
• In this way, according to age and symptom signs, oral glucose electrolyte solution is given orally every 2 to 4 hours for 12 to 24 hours for rehydration therapy and status maintenance hydration therapy.
Depending on the concentration of sodium ions (Na⁺) in the blood, dehydration is classified as follows.
1. Isotonic Dehydration – When the concentration of sodium ions (Na⁺) in the blood is normal, dehydration is called isotonic dehydration,
2. Hypertonic Dehydration – Dehydration when the blood concentration of sodium is higher than normal is referred to as hypertonic dehydration,
3. Hypotonic Dehydration – Dehydration when the blood concentration of sodium is lower than normal is called hypotonic dehydration. Mild dehydration usually occurs when one or two meals are missed or missed for some reason or another, and isotonic dehydration is likely.
Table 32. Assessment of Dehydration Severity in Infants and Infants degree of dehydration 표 32. 영유아들의 탈수 중증도 평가
| Degree of dehydration | |||
| Content of observation or examination | Mild dehydration (5%) | Moderate dehydration (10%) | Severe dehydration (15%) |
| General condition | Thirst, anxiety, excitement | Thirst, anxiety, irritability | Withdraw, Atrophy, lethargy, lethargy, rapid and deep breathing |
| Pulse | Normal | Fast | More faster |
| Pulse condition | Normal | Weak | Weak and difficult to palpate |
| Anterior fontanel feeling | Normal | Sunken | More sunken |
| Eyeball | Normal | Sunken | More sunken |
| Teardrop in crying | Tear | No tear | No tear |
| Mucous membranes and lips | Slight dry | Dry | Drier |
| Skin tension | Normal | Decreased | Further reduced or tented |
| Touch the skin | Normal | Dry | Drier |
| Urine | The amount can be normal | Decreased in quantity and high in concentration | Not urinating for several hours |
| Time to fill capillaries | Normal | Within 2 seconds | Take more than 3 seconds |
| Weight loss | 4~5% | 6~9% | 10% or more |
출처: Infectious Diseases In Children P18, Vol 17 #5 May 2004 & CDC
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
표 33. 등장성 탈수증, 저장성 탈수증, 고장성 탈수증의 증상 징후
Symptoms, signs of isotonic dehydration, hypotonic dehydration and hypertonic dehydration
| – | Isotonic dehydration | Hypotonic dehydration | Hypertonic dehydration |
| Serum sodium (Na+) concentration (mEq/L) |
Concentration of serum sodium ions (Na⁺) 130~150 (mEq/L) |
Concentration of serum sodium ions (Na⁺) 130 (mEq/L) or less |
Concentration of serum sodium ions (Na⁺) 150 (mEq/L) or more |
| Skin color | Gray | Gray | Gray |
| Skin temperature | Cold | Cold | Cold |
| Skin turgor | abnormal | Very abnormal | Very abnormal |
| Skin feeling | Dry | Wet feeling | The feeling of touching the dough
|
| Mucous membrane | Dry | Dry | Very dry |
| Eyeball | Sunken | Sunken | |
| Anterior fontanel | Sunken | Sunken | Sunken |
| Mental state | Bad | Bad | Very bad |
| Decrease in blood pressure | Decreased | Somewhat decreased | Very much decreased |
Signs, symptoms of mild dehydration
• lack of energy,
• Decreased urine output;
• Urination interval is longer than usual,
• Abnormally reduced frequency of urination
• thirst
Table 29 Daily water and Na⁺ and K⁺ electrolyte ions required per 100 calories for each symptom or disease Average water and electrolyte requirements per 100 calories per 24 hours
표 29 각 증상이나 병에 따른 100칼로리 당 필요한 1일 수분과 Na⁺, K⁺ 전해질 이온의 필요량
Average water and electrolyte requirements per 100 calories per 24 hours
| Disease name, symptom, clinical condition | H2O (물) (mL) | Na+ mEq | K+ mEq |
| Average Extraintestinal Fluid Needs | 100-120 | 2-4 | 2-3 |
| 0 | 0 | ||
| Acute central nervous system infection and inflammation | 80-90 | 2-4 | 2-3 |
| Diabetes insipidus | 400까지 | Change from time to time | Change from time to time |
| Hyperventilation | 120-210 | 2-4 | 2-3 |
| Fever. stress | 120-240 | Change from time to time | Change from time to time |
| High humidity environment | 80-100 | 2-4 | 2-3 |
• During rehydration treatment with intravenous glucose electrolyte solution and status maintenance hydration treatment, if there are no symptoms such as diarrhea, vomiting, abdominal pain, and overall improvement in severity, the dose of intravenous glucose electrolyte solution rehydration maintenance treatment is gradually reduced. Stop the glucose electrolyte solution injection last.
• Conversely, the maintenance therapeutic dose of oral glucose electrolyte solution is gradually increased.
• After that, no longer give an injectable glucose electrolyte solution or an oral glucose electrolyte solution when the vomiting diarrhea is no longer present.
• From this point on, whether breastfeeding only, artificial nutrition without lactose, beef broth, or chicken broth, one or two semi-fluid foods or full-flow foods, depending on age, are carefully selected for the next 12 to 24 hours. eat.
• Then vomiting, diarrhea, or stomach pain with little or no signs of stomach pain, but at the stage when gastroenteritis is almost recovered When there are no signs of symptoms and you are healthy, you start eating your usual food.
• It is common to be hospitalized for two to three days or longer to be treated this way.
• Do not eat milk or foods containing milk or lactose for the first 2 to 3 days, sometimes 1 to 2 weeks, after gastroenteritis has cleared.
• Of course, the cause is treated at the same time.
• This treatment is part of professional vomiting diarrhea dehydration treatment, but parents should know. And do it as directed by your doctor.
Figure 104. If severely dehydrated due to vomiting, diarrhea, etc., it is treated with glucose electrolyte solution injection. Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
Kind and composition of oral electrolytes solutions for treatment of diarrhea and, or vomiting
• Oral glucose electrolyte solution can be used to treat diarrhea, vomiting, dehydration, gastroenteritis, etc. in children and young children, especially in infants.
• Electrolyte solutions that can be used to treat vomiting, diarrhea and dehydration include oral, vascular and, rarely, bone marrow injections.
• Oral glucose electrolyte solutions are commonly used to treat dehydration, either for rehydration therapy, or for status quo hydration.
① Hydration treatment with oral glucose electrolytes solution for vomiting and, or diarrhea
• Parents may initiate oral hydration therapy with an oral glucose electrolyte solution at home when children and adolescents, especially infants, have mild gastroenteritis with mild vomiting and/or diarrhea and mild dehydration.
• Oral rehydration therapy or status quo hydration solution is called oral glucose electrolyte solution, ionic liquid, or ionized water.
• Glucose electrolyte powders are available instead of solutions.
• You can obtain an oral glucose electrolyte solution from a pharmacy without a doctor’s prescription and use it at home when mild diarrhea, vomiting, and dehydration occur in young children according to the directions written there.
• You can also treat dehydration caused by gastroenteritis by making an oral sugar electrolyte solution at home as prescribed by your doctor (see Table 3).
Picture 101. Pedialite is a kind of oral glucose electrolyte solution. It can be used for rehydration treatment or status maintenance hydration treatment when there are symptoms such as vomiting and/or dehydration caused by diarrhea. There are many similar oral glucose electrolyte solutions. It can also be purchased at a pharmacy or supermarket without a doctor’s prescription (see Table 3). Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Table 3. Oral electrolyte rehydration, status quo hydration solution for the treatment of acute diarrhea and dehydration.
표 3. 급성 설사와 탈수의 치료에 쓸 수 있는 경구용 전해질 재수화, 현상유지 수화 용액.
| Types of Oral Glucose Electrolyte Solution | Na+ in nM/L | K+ in nM/L | Cl– in nM/L | HCO3– mEq/L | glucoe/L(%) | mos M |
| Oral rehydration solution primarily used for emergency treatment of diarrhea and dehydration | ||||||
| Oral Rehydration Solution recommended by WHO | 90 | 20 | 80 | 30 | 111(2%) | 310 |
| Rehydrate solution) | 75 | 20 | 65 | 30 | 139(2.5%) | 305 |
| Oral maintenance solution used to prevent further dehydration (oral glucose electrolyte solution) | ||||||
| Infalyte (Pennwalt company) | 50 | 20 | 40 | 30 | 111(2%) | 270 |
| Pedialyte (Ross Company) | 45 | 20 | 35 | 30 | 139(2.5%) | 250 |
| Ricelyte (Mead Johnson Company) | 50 | 25 | 45 | – | 3(%) | – |
| Types and ingredients of whole formulas that should not be used as rehydration or maintenance solutions | ||||||
| 가타라데 (Gatorade) | 23 | 3 | 17 | 3 | 255 | 330 |
| 콜라(Cola) | 2 | 0.1 | 2 | 13 | 730 | 750 |
| 쿨에이드(Kool-Aid) | 3 | 0.1 | 0 | 0 | 105 | 465 |
| 사과주스 (Apple juice) | 3 | 28 | 30 | 0 | 690 | 725 |
| 하이시(Hi-C) | 2 | 5 | 0 | 0 | 800 | 816 |
| 폽씨클 (Popsicle) | 5 | 0.5 | 0 | 0 | 710 | 719 |
| 닭고기 국물
Chicken broth |
251 | 8 | 250 | 0 | 0 | 501 |
| Water | 0 | 0 | 0 | 0 | 0 | – |
주: 적절한 현상 유지 수화 치료용액은 5-10% Dextrose와 0.2% NaCl + 20 mEq/L KCl 또는 K acetate이다.
참고: 경구용 포도당 전해질 현상유지 용액과 재수화 용액은 비 의료인들이 의사의 처방 없이 약국이나 수퍼마켓트에서 사서 쓸 수 있게 법으로 정하면 좋을 것이라고 생각한다.
표 30. 각종 체액의 전해질 이온 성분, 수소이온 농도(pH)와 삼투압 Electrolytes, pH, Osmolarity of body fluids
| Blood or body fluids | Na+ | K+ | Cl– | HCO3– | pH | Osmotic pressure |
| Gastric juice | 50 | 10~15 | 150 | 0 | 1 | 300 |
| Panceatic juice | 140 | 5 | 50~100 | 100 | 9 | 300 |
| Bile | 130 | 5 | 100 | 40 | 8 | 300 |
| Ileostomy opening serous fluid obtained from | 130 | 15~20 | 120 | 25~30 | 8 | 300 |
| Diarrhea stool | 50 | 35 | 40 | 50 | alkalinity | |
| Sweat | 50 | 5 | 55 | 0 | – | – |
| Blood | 140 | 4~5 | 100 | 25 | 7.4 | 285~295 |
| Urine | 0~100 | 20~100 | 70~200 | 0 | 4.5~8.5 | 50~1400 |
Note: A suitable maintenance hydration treatment solution is 5-10% Dextrose and 0.2% NaCl + 20 mEq/L KCl or K acetate.
Note: I think it would be good if the law stipulates that non-medical people can buy glucose electrolytes and rehydration solutions for oral use at pharmacies or supermarkets without a doctor’s prescription.
• As shown in Table 30, electrolyte components and ion concentrations in body fluids in each organ of each system are different.
• In particular, among the electrolyte components of body fluids of each organ, K⁺, H⁺, Cl⁻, Na⁺, and HCO3⁻ are normally different.
• It is common to treat dehydration when you have diarrhea, sweat a lot, and consider which electrolytes are lost and how much.
• Dehydration due to diarrhea Do not treat dehydration caused by diarrhea or vomiting with freshwater or barley tea containing little electrolyte.
Figure 90. When the intestinal wall mucosal layer is damaged or swollen, causing diarrhea Electrolytes such as K⁺ (potassium (potassium) ion), H⁺ (hydrogen ion), Cl⁻ (chloride ion), Na⁺ (sodium ion), HCO3⁻ (bicarbonate ion) and undigested food in the small intestine and intestinal juices may be excreted in the feces. For this reason, dehydration caused by diarrhea or vomiting should not be treated with plain water or barley tea water, which contains little electrolyte. Copyright© 2001 John Sangwon Lee, MD.FAAP
◆ See sources and references
① Acute dehydration
② Electrolytes, pH, and osmolarity of body fluids in each system
③ Isotonic dehydration
④ Dehydration evaluation in infants and children ⑤ Symptomatic signs of isotonic dehydration, hypotonic dehydration, and hypertonic dehydration
⑥ Can be used to treat diarrhea and dehydration Acute dehydration oral rehydration solution; oral maintenance solution; Comparison table of electrolyte concentration, glucose concentration, and osmotic pressure in clear liquid diets
⑦ Average water and electrolyte required per 100 calories per day requirements per 100 calories per 24 hours)
⑧ Acidosis (Acidosis)
⑨ Acute dehydration due to diarrhea, vomiting ⑩ Causes and mechanism of diarrhea and/or vomiting
⑪ Diarrhea and vomiting caused by infectious diseases ⑫ Food for diarrhea
⑬ Diarrhea Vomiting and medication (Drug treatments for diarrhea and vomiting)
⑭ Oral hydration electrolyte solutions
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서
Copyright ⓒ 2014 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine.